what drugs are used to treat parkinsons disease
Introduction [edit | edit source]
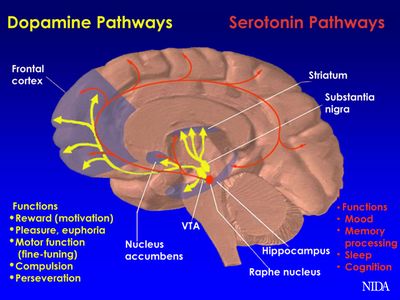
Parkinson's is a progressive neurodegenerative disorder that affects motor part. This disease has go an epidemic, affecting approximately 1 percent of individuals over the age of 65 years sometime [1]. It is caused past decreased dopamine production in the basal ganglia due to degeneration of dopamine-secreting neurons [two],[iii].
Initially, people with Parkinson's may be asymptomatic with the outset clinical symptoms appearing afterwards 60% of the dopaminergic neurons accept degenerated in the substantia nigra [4]. Central symptoms of Parkinson illness include bradykinesia, akinesia, rigidity, and resting tremors [2],[5]. The exact cause of Parkinson'southward is unknown; however, contributing factors to may include trauma, infection, cortical degeneration, antipsychotic drugs and cerebrovascular affliction [half dozen] [7] [viii] [9]. If Parkinson's goes untreated, total incapacitation will occur due to uncontrolled motor bug. This is why it is extremely of import for Parkinson'due south patients to be prescribed the proper drug regimen. The video below outlines briefly medication rational and major drug types
[ten]
The inter-dependency of healthcare professionals is significant in the management of Parkinson's. Specialists are encouraged to take the knowledge and understanding of the condition and its impact on the quality of life. Communication is a key and it should aim to empower individuals who suffer Parkinson's to develop effective self-direction strategies with an optimistic and realistic arroyo.
Understanding the touch on of medication on both the movement and thought quality of people with Parkinson's volition aid ready goals and plans for physiotherapy intervention. Individual Parkinson's Associations provide country-specific information about medications prescribed. Due east.g. In the Uk, where physiotherapists can railroad train to prescribe medication, a skillful summary of drug therapies tin can be found on the Parkinson'due south U.k. site and in the US, the National Parkinson'southward Foundation provides communication.
Parkinson'south medications are almost usually administrated orally. Injections and subcutaneous medications are available only expensive.
Medication aid in controlling motor and not-motor symptoms, however, fluctuations in the responsiveness are experienced as the status is progressed. Wearing off and motor fluctuations occur every bit the body develops dependency and the threshold to medications is altered. Refer to the EPDA website to learn more on wearing off.
Deep brain stimulation, stem cell therapy and gene therapy are alternative approaches that aim to lower the need to medications.
The primary types of drugs that are used to treat Parkinson'south are[xi]: [edit | edit source]
- Levodopa
- Dopamine agonists
- Glutamate antagonist
- Anticholinergics
- COMT inhibitors
- MAO-B inhibitors
- Dopaminergic Medications
Levodopa [edit | edit source]
Levodopa (50-dopa) is a common drug administered during the progressive stages of PD. 50-dopa is considered a prodrug, pregnant it is not activated until after it crosses the blood brain bulwark via active transport[12]. The primary utilise of Levodopa is to restore depleted levels of dopamine at the presynaptic terminal of the substantia nigra, which restores functional move[xiii]. This replacement tin can relieve symptoms of PD, such as freezing and rigidity[14]. If a tolerance is built upwards to L-dopa, or adverse motor effects go present with this drug alone, partner drugs Benserazide and Carbidopa (LD-CD) tin be supplemented to prevent the farther premature breakdown in the periphery[15].
Optimal oral dosing of LD-CD is typically between 97.5 mg-390 mg for a single dose, and 25mg-100mg bi-daily/tri-daily for either sustained release or immediate release[16]. The book of distribution is typically around 28.5 50 and the plasma half-life clearance is 1.eight hours. Therefore, frequent dosage is required. The renal clearance of L-dopa is approximately 72 ml/min[13].
Many of the agin effects that are present with Levodopa are due to the fact that it is not combined with a partner drug. Some of the most mutual adverse effects to be aware of during a concrete therapy visit include gastrointestinal distress due to the enteral administration, cardiac difficulties, gait disturbances due to dyskinesias, terminate of dose akinesia, and a tolerance subsequently around 3-4 years. Administering physical therapy treatment during the peak time of this drug helps to avoid these end of dose side effects[14].
MAO-B Inhibitors [edit | edit source]
Monoamine Oxidase B Inhibitors, such as Selegiline and Rasagiline, are unremarkably used by patients with Parkinson'due south considering of their potential disease modifying and neuroprotective effects [17]. This drug course is considered a potential affliction modifier due to its power to inhibit the monoamine oxidase type B (MAO-B) enzyme, which naturally breaks downward dopamine in the brain[17].By inhibiting the breakup of the MAO-B enzyme, these drugs are able to extend the effects of dopamine at the CNS synapse [18] [xix]. However, more research needs to exist done on the ability of MAO-B inhibitors to boring the progression of PD. MAO-B inhibitors exhibit neuroprotection by decreasing dopamine oxidation, therefore preventing excessive product of free radicals, while prolonging the furnishings of endogenous dopamine[20] [21] MAO-B inhibitors can exist used as an initial drug in the handling of Parkinson'southward Disease or tin be combined with Levodopa in order to reduce motor fluctuations[17].
The prototypical selective, irreversible MAO-B inhibitor, Selegiline, is captivated in the GI tract and so distributed to tissues throughout the body, including the encephalon[22]. Selegiline is metabolized to L-amphetamine-similar metabolites which may promote insomnia [17]. This drug is primarily metabolized in the liver and then excreted past the kidneys [22]. Selegiline has an oral bioavailability of 10% and an oral clearance rate of 59 50/min [23]. This drug is given at a therapeutic dose of 10mg/twenty-four hours and has a half-life of 10 hours[17]. Selegiline is typically administered twice per day as a 5mg oral tablet [24]. If this dose is increased Selegiline volition lose it'south selective ability[17].
Rasagiline, another selective, irreversible MAO-B inhibitor, is metabolized into aminoindan in the liver by cytochrome p450 type 1A2, which means it does not have the amphetamine-similar effects that Selegiline displays and may be preferred[25]. Its oral bioavailability is 35% and it reaches its therapeutic maximum subsequently 0.v-ane hour [25]. The oral clearance rate of Rasagiline is 94.iii 50/mean solar day[25]. This drug is given at a recommended dose of 0.5-1 mg/day and has a half-life or 1.v-three.v hours [25]. It is typically administered once per day as a 0.5mg or 1mg oral tablet [24].
When used in adjunct with Levodopa both Selegiline and Rasagiline have been known to decrease motor fluctuations in patients with Parkinson'south [17]. These 2 drugs are relatively safe compared to other MAO inhibitors due to their selective ability[26]. Mutual agin effects of other MAO-B Inhibitors may include dizziness, headache, GI distress, and sedation[26].
Dopamine Agonist Medications [edit | edit source]
Dopamine agonists are another ordinarily used form of drugs implemented during the handling of PD[27] [28]. Dopamine agonists work past actively influencing dopamine receptors in the encephalon to produce more in-vivo dopamine, thus making information technology the preferential treatment early on in the affliction process. Apomorphine is considered the premier drug in this category, due to its powerful motor fluctuation modulating capabilities, such every bit those seen in finish of dose dyskinesias generated by some anti-parkinsonian medications (i.e. LD)[29]. Apomorphine is typically administered subcutaneously on a continuous wheel for an boilerplate of 16 hours per day at a rate of iii-6 mg/60 minutes[xxx]. Further pharmacokinetics of apomorphine, include the drug taking approximately 15-twenty minutes to accomplish its maximum bioavailability within the bloodstream[31] [32]. Once in the blood, the drug takes nearly 30-twoscore minutes to reach its half life[30] [31] [32]. This is adequately quick and the reason for the drug beingness given on a abiding basis throughout the day[30]. Apomorphine'due south clearance in the organization is close to iii-4 L/h/kg, significant that it leaves the plasma at a rapid rate[33]. After the drug has been metabolized, it is then excreted through urine by the kidneys[xxx].
The main adverse effects seen after the intake of this medication include somnolence, withdrawal, and psychiatric disorders, such equally confusion and hallucinations[29] [30]. Information technology is vital that the physical therapist is aware of such side effects to dictate the treatment.
Anticholinergic Medications [edit | edit source]
Anticholinergic drugs, including Benztropine mesylate, Biperiden, Diphenhydramine, and Trihexyphenidyl, are some other important class of medications used to mitigate the motor symptoms of Parkinson's affliction. By using these drugs in the early progression of the disease, the need for Levodopa can exist prolonged. While the exact machinery of activeness is unknown, it is said that anticholinergic drugs are competitive antagonists of muscarinic receptors; thus, inhibiting disproportionate acetylcholine activeness from the basal ganglia, specifically involuntary muscle motion. These drugs are taken orally and range from thirty-seventy% bioavailable. After taken, they are rapidly absorbed (with the exception of benztropine mesylate) into the brain and produce a high volume of distribution, then biotransforming via N-dealkylated and hydroxylated metabolites. The drug clearance appears to exist low in comparison to hepatic blood flow, which reduces the chances of first pass effect. Excretion of the parent drug and metabolite are through the kidneys. With these things being said, at that place is very little data on the pharmacokinetic data for anticholinergic drugs.
As for dosage, the suggested amount of this class of drugs is between six-xx mg daily; however, in that location is a specific anticholinergic phenothiazine compound that is to be taken from 50-600 mg daily. The one-half life of anticholinergic drugs is between 4 hours to 24 hours, with Diphenhydramine beingness on the shorter range and Biperiden existence on the higher range.
Each medication has its own particular side effects; notwithstanding common agin effects of anticholinergic drugs include memory bug, drowsiness, constipation, sedation, urinary retentivity, blurred vision, tachycardia, and delirium. Increased side effects are typically seen in the elderly, when compared with younger adults. As a physical therapist, these are all things to consider, especially when treating your elderly patients. Futurity studies must be performed to go a better understanding of why elderly patients tolerate this drug less[34].
References [edit | edit source]
- ↑ Harris PE ,C. Chiliad. Prevalence of complementary and alternative medicine (CAM) used by the general population: a systematic review and update. NCBI. https://www.ncbi.nlm.nih.gov/pubmed/22994327. October, 2012. Accessed Nov 5, 2018.
- ↑ 2.0 two.1 Chen JJ, Nelson MV, Swope DM. Parkinson's disease. DiPiro JT, Et al, eds. Pharmacotherapy: A Pathophysiologic Arroyo. 8th ed. New York: Mcgraw-Colina. 2011.
- ↑ Parent M, Parent A. Substantia nigra and Parkinson's: a brief history of their long and intimate relationship. NCBI. https://www.ncbi.nlm.nih.gov/pubmed/20481265. May, 2010. Accessed November v, 2018.
- ↑ Lecht, S., Haroutiunian, S., Hoffman, A., & Lazarovici, P. Rasagiline – A Novel MAO B Inhibitor in Parkinson's Disease Therapy. NCBI. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2386362/. June, 2007. Accessed Nov 5, 2018.
- ↑ Garcia Ruiz PJ, Catalan MJ, Fernandez Carril JM. Initial motor symptoms of Parkinson disease. NCBI. https://www.ncbi.nlm.nih.gov/pubmed/22045320. November 17, 2011. Accessed November 5, 2018.
- ↑ Gelabert-Gonzalez 1000, Serramito-Garcia R, Aran-Echabe Due east. Parkinsonism secondary to subdural haematoma. NCBI. https://www.ncbi.nlm.nih.gov/pubmed/22527627. July, 2012. Accessed November 5, 2018.
- ↑ Gupta D Kuruvilla. Vascular parkinsonism: what makes it different? NCBI. https://world wide web.ncbi.nlm.nih.gov/pubmed/22121251. Dec, 2011. Accessed November 5, 2018.
- ↑ Lopez-Sedon JL, Mena MA, de Yebenes JG. Drug-induced parkinsonism in the elderly: incidence, management and prevention. NCBI. https://www.ncbi.nlm.nih.gov/pubmed/22250585. February, 2012. Accessed November 5, 2018.
- ↑ Mazokopakis EE, Koutras A, Starakis I, Panos Chiliad. Pathogens and chronic or long-term neurologic disorders. NCBI. https://www.ncbi.nlm.nih.gov/pubmed/21446901. March, 2011. Accessed November 5, 2018.
- ↑ PD care New York Taking Control: Medications for Parkinson's Available from: https://www.youtube.com/sentinel?v=T8VojsSvv4E (last accessed 8.11.2019)
- ↑ Parkinsons Victoria Medications Available from: https://world wide web.parkinsonsvic.org.au/parkinsons-and-you/medications/ (terminal accessed 7.11.2019)
- ↑ Standaert DG, Roberson ED. Chapter 22: Handling of Fundamental Nervous System Degenerative Disorders. In: Goodman & Gilman's: The Pharmacological Basis of Therapeutics. Vol 1. 12th ed. New York, NY: The McGraw-Loma Companies, Inc. ; 2011.one.
- ↑ 13.0 13.1 Lewitt Medico, PA. Levodopa therapy for Parkinsons disease: Pharmacokinetics and pharmacodynamics. Movement Disorders. 2014;xxx(1):65-67. doi:10.1002/mds.26082.
- ↑ 14.0 xiv.ane Connolly MD, BS, Lang Medico, AE. Pharmacological Handling of Parkinson Illness. Jama. 2014;311(xvi):1670. doi:10.1001/jama.2014.3654.
- ↑ del Amo EM, Urtti A, Yliperttula G. Pharmacokinetic role of 50-type amino acid transporters LAT1 and LAT2. European Journal of Pharmaceutical Sciences. 2008;35(iii):161-174. doi:ten.1016/j.ejps.2008.06.015
- ↑ Hsu A, Yao HM, Gupta Due south, Modi NB. Comparison of the pharmacokinetics of an oral extended‐release capsule formulation of carbidopa‐levodopa (IPX066) with immediate‐release carbidopa‐levodopa (Sinemet®), sustained‐release carbidopa‐levodopa (Sinemet® CR), and carbidopa‐levodopa‐entacapone (Stalevo®). The Periodical of Clinical Pharmacology. 2015 Sep i;55(nine):995-1003.
- ↑ 17.0 17.1 17.2 17.3 17.iv 17.v 17.six Teo KC, Ho SL. Monoamine oxidase-B (MAO-B) inhibitors: implications for disease-modification in Parkinson's illness. Translational neurodegeneration 2013 Dec;2(1):nineteen.
- ↑ Fabbrini Yard, Abbruzzese M, Marconi S, Zappia Chiliad. Selegiline: a reappraisal of its role in Parkinson disease. Clinical neuropharmacology 2012 May 1;35(iii):134-forty.
- ↑ Magyar K. The pharmacology of selegiline. In: International review of neurobiology. Academic Press, 2011 (Vol. 100, pp. 65-84).
- ↑ Weinreb O, Amit T, Bar-Am O, Youdim MB. Rasagiline: a novel anti-Parkinsonian monoamine oxidase-B inhibitor with neuroprotective activity. Progress in neurobiology 2010;92(iii):330-44.
- ↑ Aluf Y, Vaya J, Khatib S, Loboda Y, Finberg JP. Selective inhibition of monoamine oxidase A or B reduces striatal oxidative stress in rats with partial depletion of the nigro-striatal dopaminergic pathway. Neuropharmacology 2013;65:48-57.
- ↑ 22.0 22.one Heinonen EH, Myllylä 5, Sotaniemi 1000, Lamintausta R, Salonen JS, Anttila 1000, Savijärvi M, Kotila M, Rinne UK. Pharmacokinetics and metabolism of selegiline. Acta neurologica Scandinavica. Supplementum 1989;126:93-9.
- ↑ Mahmood I. Clinical pharmacokinetics and pharmacodynamics of selegiline. Clinical pharmacokinetics 1997;33(2):91-102.
- ↑ 24.0 24.1 UCSF School of Medicine. Parkinson's Clinic and Research Center. Available from: http://pdcenter.neurology.ucsf.edu/patients-guide/parkinson's-affliction-medications/monoamine-oxidase-b-mao-b-inhibitors(accessed 5 November 2018).
- ↑ 25.0 25.1 25.2 25.three Lecht S, Haroutiunian Southward, Hoffman A, Lazarovici P. Rasagiline–a novel MAO B inhibitor in Parkinson'southward affliction therapy. Therapeutics and clinical risk management 2007;three(iii):467.
- ↑ 26.0 26.ane Chen JJ, Wilkinson JR. The monoamine oxidase blazon B inhibitor rasagiline in the treatment of Parkinson affliction: is tyramine a challenge? The Periodical of Clinical Pharmacology 2012 May;52(v):620-8.
- ↑ Bonuccelli U, D. D. Role of dopamine receptor agonist in the treatment of early Parkinson's. Parkinsonism Related Disorders, 2009;(4): S44-53.doi: ten.1016/S1353-8020(09)70835-1.
- ↑ Harris PE ,C. K. Prevalence of complementary and alternative medicine (CAM) used by the general population: a systematic review and update. Int J Clin Pract, 2012; 66(10): 924-939. doi: 10.1111/j.1742-1241.2012.02945.x.
- ↑ 29.0 29.1 Regina Katzenschlager Physician, W. P. Apomorphine subcutaneous infusion in patients with Parkinson'due south with persistent motor fluctuations (TOLEDO): a multicentre, double-blind, randomised, placebo-controlled trial. The Lancet Neurology, 2018;(ix):749-759. doi: 10.1016/S1474-4422(eighteen)30239-
- ↑ 30.0 30.1 30.2 30.3 xxx.4 Auffret K, D. Southward. (2018) Pharmacological Insights into the Utilise of Apomorphine in Parkinson's: Clinical Relevance. Clinical Drug Investigation, 2018; 38(4) 287-312. doi: 10.1007/s40261-018-0619-3.
- ↑ 31.0 31.1 Nomoto Thousand, Kubo SI, Nagai Grand, Yamada T, Tamaoka A, Tsuboi Y, Hattori N, Parkinson's Study Group. A randomized controlled trial of subcutaneous apomorphine for Parkinson disease: a repeat dose and pharmacokinetic study. Clinical neuropharmacology. 2015 Nov 1;38(6):241-7.
- ↑ 32.0 32.i Elisa Unti, R. C. Apomorphine hydrochloride for the treatment of Parkinson'south . Skillful Review of Neurotherapeutics, 2015; 15(7): 723-732. doi: 10.1586/14737175.2015.1051468.
- ↑ rgiolas A, H. H. (2001). The pharmacology and clinical pharmacokinetics of apomorphine. BJU international, 2001; 88(3): 18-21. https://doi.org/ten.1046/j.1464-4096.2001.00124.ten
- ↑ Brocks, D. R. Anticholinergic drugs used in Parkinson's: An disregarded class of drugs from a pharmacokinetic perspective. J Pharmaceut Sci.https://sites.ualberta.ca/~csps/JPPS2(2)/D.Brocks2/anticholinergic.htm. Baronial 22, 1999. Accessed November 5, 2018
Source: https://www.physio-pedia.com/Drugs_for_the_Treatment_of_Parkinson%27s
0 Response to "what drugs are used to treat parkinsons disease"
Post a Comment